

Intrauterine insemination with ovarian stimulation versus expectant management for unexplained infertility (TUI): a pragmatic, open-label, randomised, controlled, two-centre trial
不明原因不孕妇女子宫内人工授精联合卵巢刺激与期待疗法的比较(TUI):一项实用、开放、随机、对照、双中心试验
翻译:深圳市第二人民医院 生殖医学科 汪丽萍、胡晴钰
一、文献解析
1、背景介绍
不明原因不孕的夫妇通常会接受宫内授精(IUI)和卵巢刺激方案,在美国、英国和欧洲广泛使用,作为不明原因不孕夫妇体外受精(IVF)的一种低成本、侵入性较小的替代方案。然而,很少有证据表明IUI是一种有效的治疗方法。2013年,英国国家健康和护理卓越研究所(NICE)建议,无论是否有卵巢刺激,IUI都不应该常规提供给不明原因不孕的夫妇,而是可以在期待疗法(EM)两年后考虑IVF。然而,一项2015年英国不孕不育的临床报道指出对96%的人继续提供IUI。
在开始这项研究之前,我们在Cochrane Library和PubMed上搜索了从数据库开始到2012年12月3日以英语发表的相关研究。我们使用了以下搜索术语:“原因不明的不孕症”、“原因不明的低生育力”、“子宫内人工授精”、“子宫内输卵管妊娠人工授精”、“IUI”、“伴侣人工授精”和“人工授精”。我们确定了一个高质量的Cochrane系统综述,没有额外的试验。Cochrane系统综述报道了两项比较IUI和EM的随机对照试验,两项研究都没有报道哪种方法更可靠。本项研究是一项可靠的随机对照试验,对未来12个月内自然受孕预后不良的妇女进行IUI和枸橼酸氯米芬与期待疗法进行比较。与该领域以前的随机对照试验不同,我们研究预后不良,并且使用了枸橼酸氯米芬诱导排卵。临床上对原因不明的不孕不育症,IUI 通常与促排卵药物一起作为原因不明不孕不育症的首选治疗手段。本研究是首次报道卵巢刺激IUI与期待疗法相比较可靠的研究。
本研究为一项实用、开放、随机、对照、双中心试验,旨在探讨对不明原因不孕且未来12个月内自然受孕预测评分不理想(< 30%)的妇女,比较3个周期IUI联合卵巢刺激(口服枸橼酸氯米芬或来曲唑)与3个周期EM的有效性。我们希望验证IUI卵巢刺激组的活产率更高的假设。


2、名词解释
TUI(the Uterine Insemination): 子宫授精试验。
IUI(intrauterine insemination):宫内人工授精。宫内授精(IUI)是一种人工授精,可以治疗不孕不育症,在女性排卵期,将经过清洗和浓缩的精子直接置入子宫,并与卵巢释放的一个或多个等待受精的卵子结合,期望的宫内授精结果是精子游入输卵管并让等候的卵子受精,从而怀孕。根据不孕不育症的原因,可以将 IUI 与患者正常月经周期或生育药物进行协调。
IVF(in-vitro fertilisation ):体外人工受孕。是将卵子与精子取出,在人为操作下进行体外受精,并培养成胚胎,再将胚胎植回母体内,整个过程真正在试管内的时间只有 2-6 天而已。以目前的技术,尚无法在体外将胚胎培养至足月。利用体外受精技术生产出来的婴儿称为试管婴儿(Test tube baby)。
EM(expectant management):期待疗法。
CLBR(cumulative livebirth rate):累计活产率。累积活产率的概念被逐渐推广,即综合考虑患者基线情况以及多次移植周期之间关系,进而评价患者经历多次移植后至少获得一次活产的概率大小。然而现阶段关于活产率尤其是累积活产率的研究主要集中于西方国家,对于我国,虽然周期活产率研究较为广泛深入,但是累积活产率研究尚未广泛开展,更缺乏多中心、大样本人群数据的比较。除此之外,我国辅助生殖治疗虽起步较晚但发展迅速,可开展辅助生殖治疗的获批中心数量呈现逐年上升趋势,客观上有可能造成诊疗方案和治疗水平在地区上的不平衡。因此,对不同中心不同辅助生殖治疗效果、活产率的研究亟待开展。
NICE(The UK National Institute for Health and Care Excellence ):英国国家健康与护理卓越研究所。

3、方法设计
子宫授精(TUI)研究是一项实用、开放、随机、对照、双中心的研究,研究对象为不明原因不孕且自然受孕预后不良的女性。本研究收集了所有夫妇的以下数据:年龄、体重指数、吸烟(是否)、种族、既往活产、既往IVF或IUI周期、不孕持续时间、无排卵性多囊卵巢综合征和轻度子宫内膜异位症的诊断、抗苗勒管激素水平、精子计数和活动力以及未来12个月自然受孕的Hunault预测评分。对于随机分配到IUI卵巢刺激组的夫妇,收集了关于刺激方案类型(克罗米芬或来曲唑)的其他数据;第12天雌二醇水平;第12天直径大于16 mm的卵泡数;使用卵巢触发剂(如果卵泡直径≥18 mm且未检测到黄体生成素升高);黄体期支持;新鲜或冷冻精子;和受精的活动精子总数。
纳入标准:本研究纳入了年龄小于42岁、体重指数小于35 kg/m2、不明原因不孕:定义为正常排卵(或卵巢刺激正常)、通过腹腔镜或子宫输卵管造影术确定双侧输卵管通畅、精液分析正常(进行性活动率≥32%、浓度≥1500万/mL)、自然受孕导致下一年活产的预测分数小于30%的女性。使用了经过验证的Hunault自然受孕预测模型,包括年龄、不孕时间、既往妊娠史、转诊来源和精子活力。我们纳入了轻度子宫内膜异位症(经腹腔镜检查确诊)、多囊卵巢综合征根据鹿特丹标准定义(假设至少6个周期内有或无卵巢刺激证实排卵)、以及既往IUI或IVF周期的妇女。
排除标准:需要供体精子的妇女。
分组方式:我们招募了在新西兰两个生育诊所就诊的不明原因不孕且自然受孕预后不良的妇女。受试者被随机分配(1:1)接受三个周期的IUI卵巢刺激(口服枸橼酸氯米芬[50-150mg,第2-6天]或口服来曲唑[2.5-7.5mg,第2-6天],卵巢刺激由诊所选择)或三个周期的期待治疗(建议夫妇在可能的排卵时间进行性活动,并提供日记记录每个月经周期的第一天和性活动的日期)参与的夫妇和临床医生被告知治疗分配。
最后共纳入在2013年3月12日至2016年5月12日的201例妇女被随机分配至期待疗法组(n=100)和子宫内人工授精组(n=101),并对研究人群进行意向性分析。
干预手段:所有妇女在进入研究前都进行了筛查试验:登记前不到3年的宫颈涂片、高阴道拭子、病毒检测和风疹免疫。两家诊所使用相同的研究方案。在IUI卵巢刺激组,妇女接受口服枸橼酸氯米芬(默克雪兰诺;50–150毫克,第2–6天)或口服来曲唑(道格拉斯制药公司;2.5-7.5毫克,第2-6天) 根据患者反应进行卵巢刺激。卵巢刺激的选择由临床决定。当有1-3个卵泡时,将制备好的0-5ml精子注射入子宫进行IUI。在第7天测量雌二醇和黄体生成素。在第一个周期中,当雌二醇高于400 pmol/L时,如果在随后的周期中有临床指征,开始进行系列超声检查。当第一个卵泡直径大于等于14 mm或雌二醇达到400 pmol/L时,开始每日追踪黄体生成素。当出现1-3个卵泡时,在黄体生成素高峰后约24小时或人绒毛膜促性腺激素触发注射后36小时进行IUI。除非雌二醇水平为2000 pmol/L或更高,否则在第二或第三周期中通常不使用超声波。用雌二醇水平和超声波监测来曲唑周期。如果在授精后7天,孕酮水平低于20 pmol/L,则开始每天三次200 mg的黄体酮栓剂阴塞。授精后14天测定血清β-人绒毛膜促性腺激素。如果没有反应(雌二醇没有上升或卵泡没有发育)或如果有三个以上的卵泡(在这种情况下,要求妇女避免无保护的性交),则周期被取消。被取消的周期被另一个具有适当剂量调整的周期所替代。
研究期间,未对纳入标准或治疗干预措施进行重大方案变更。然而,由于取消、时间安排困难和早期妊娠损失,连续安排IUI和卵巢刺激周期并不总是可能的。在2014年初与数据安全监测委员会讨论后,双方同意只有在随机分组之日起6个月(185天)内完成三个IUI周期的情况下,才纳入活产儿。流产的情况例外,妇女有恢复时间,然后有时间完成分配给她们的IUI周期数。自然受孕包括在内,如果它们发生在所有三个IUI周期完成之前。如果发生宫外孕,则不再进行IUI周期。
被分配到EM组的夫妇接受了三个周期的随访。他们被建议在可能的排卵时间进行性活动,并被提供一本日记来记录每个月经周期的第一天和性活动的日期。EM组中患有无排卵性多囊卵巢综合征的妇女继续接受促排卵治疗。
主要结局:三个治疗周期后的活产率,并报告为意向性治疗人群中的累积活产率(CLBR)。
次要结局:是临床妊娠、异位妊娠、流产、多胎妊娠、卵巢过度刺激综合征、导致活产的妊娠时间和出生体重。
统计方法:对于二分变量,我们用95% CIs计算风险比(RR ),并用χ2检验检验显著性。对于连续变量,我们使用学生t检验或Kruskal-Wallis检验。我们绘制了Kaplan-Meier曲线来检测卵巢刺激IUI组和EM组之间的存活时间差异。我们用对数秩(Mantel-Cox)检验比较了这些曲线。使用IBM SPSS Statistics第23版进行分析。我们计算出,每组80名女性的样本在显著性水平为0.05(单侧检验)时将提供80%的功效,以检测CLBR 14%的差异。根据一个参与的生育诊所最近的数据,我们假设卵巢刺激IUI的CLBR为22%,子宫内膜异位症为8%。每组的最终目标是100,因为IUI卵巢刺激组的自然受孕率高于预期。我们没有按研究中心进行分层,因为我们没有预料到在同一地区的两个中心招募的妇女之间的人口统计学或临床差异。
4、图表解析
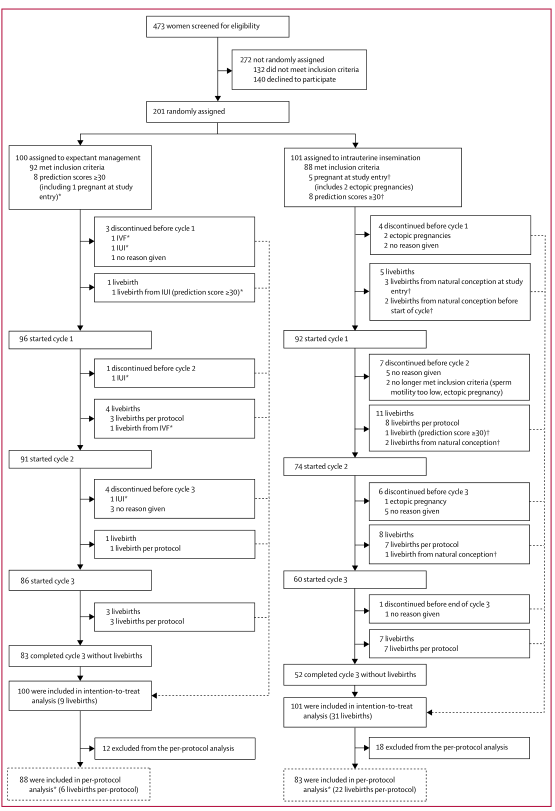
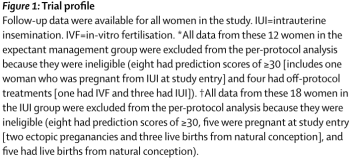
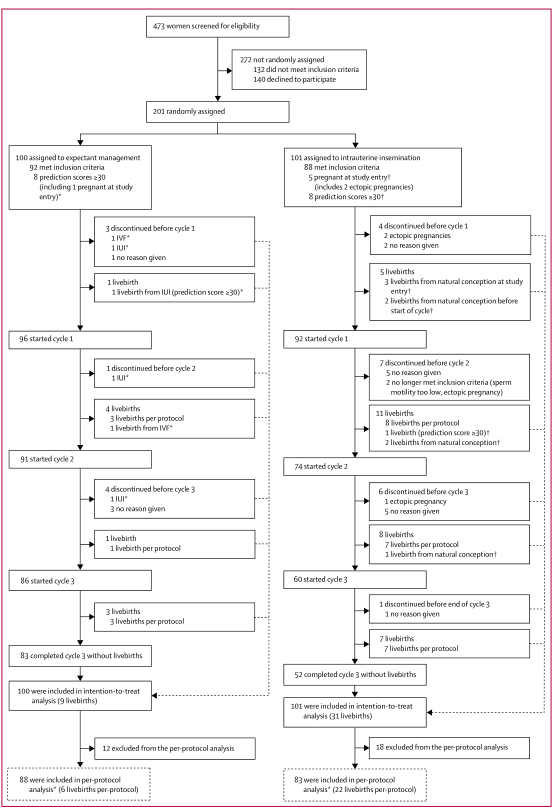
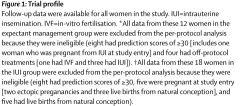
图1:试验资料。研究中的所有妇女都有试验概况随访数据,本研究共纳入473例不明原因不孕的妇女接受了资格审查,其中272例妇女不是随机分配的、132例妇女不符合纳入标准、140例拒绝参加试验,最后共纳入在2013年3月12日至2016年5月12日的201例妇女被随机分配至期待疗法组(n=100)和子宫内人工授精组(n=101),并对研究人群进行意向性分析。
*来自期待治疗组的这12名妇女的所有数据都被排除在符合方案的分析之外,因为他们不符合条件(8名预测得分≥30[包括一名在研究开始时因IUI怀孕的妇女],4名接受了不符合方案的治疗[1名进行了IVF,3名进行了IUI])。最后期待治疗组有88例纳入方案分析*(每个方案6例活产)。
†来自IUI组的这18名妇女的所有数据都被排除在符合方案的分析之外,因为她们不合格(8名预测得分≥30,5名在研究开始时怀孕[2名异位妊娠和3名自然受孕的活产儿],5名自然受孕的活产儿)。最后子宫内人工授精组有83例纳入方案分析*(每个方案22例活产)。
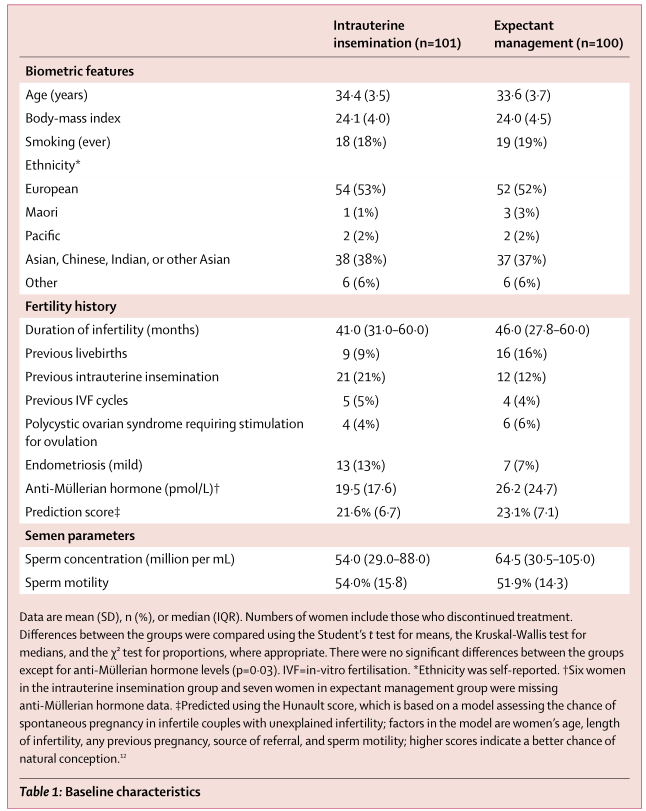
表1为接受随机分组的患者的基线特征。包括年龄、体重指数(BMI)、吸烟、人种等基本特征及生育史(不孕时间、既往活产、既往子宫内人工授精、既往体外授精周期、需要刺激的多囊卵巢综合征排卵期、轻微子宫内膜异位症、抗苗勒管激素 (pmol/L)†、预测分数‡)、精液参数(精子浓度(每毫升百万)、精子的运动性)。201例妇女的平均年龄为34岁,其中16.5%的妇女既往有子宫内人工授精,4.5%的妇女既往有体外授精周期,5%的妇女有需要刺激的多囊卵巢综合征排卵期,10%的妇女有轻微子宫内膜异位症。可以看出IUI组与EM组两组之间的基线特征相似。使用学生t 检验比较组间差异,Kruskal-Wallis 检验中位数,并在适当的情况下对比例进行 χ² 检验,除了抗苗勒管激素水平 (p=0·03),组间无显着差异。
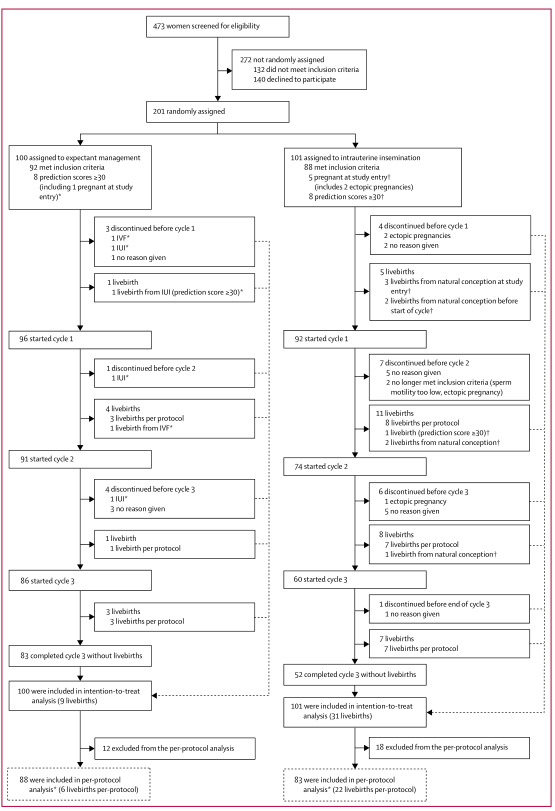
表2为妊娠结局。RR=风险比。 *一名在研究开始时怀孕的女性通过宫腔内人工授精活产,另一名活产来自第 1 周期的体外受精。 †包括研究开始时有 3 次未被识别的怀孕,周期开始前有 2 次;两次自然怀孕发生在第 1 和第 2 周期之间。‡一次自然怀孕发生在第 1 周期和第 2 周期之间。第 2 和第 3 周期。§研究开始时的两次异位妊娠。
IUI 组的活产率高于 EM 组(101 名女性中有 31 名 [31%] 活产 vs 100 名妇女中有9 名 [9%]活产; RR=3.41,95% 可信区间(1.71-6.79),p=0·0001),p<0.01,有统计学意义;IUI 组的临床妊娠率高于 EM 组(101 名女性中有 37名 [37%] 妊娠 vs 100 名妇女中有11 名 [11%]妊娠; RR=3.33,95% 可信区间(1.8-0-6.15),p<0·0001),有统计学意义。
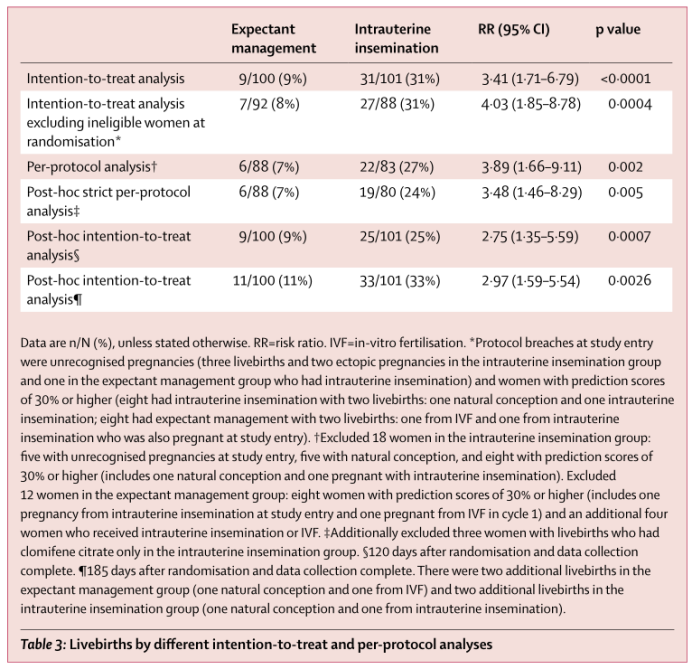
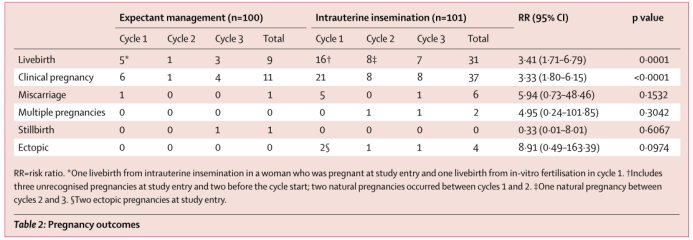
表3通过不同的意向治疗和符合方案分析的活产。IUI 组的 CLBR 高于 EM 组(101 名女性中有 31 名 [31%] 活产 vs 100 名妇女中有9 名 [9%]活产; RR=3.41,95% 可信区间(1.71-6.79);P=0·0003;表 2、3)。在 IUI 组的 31 个活产中,23 个来自 IUI 周期,3 个来自在研究开始时未被识别的怀孕,还有5个是在 IUI 周期之前或之间受孕的。在EM 组中的9个活产中,2个来自协议外治疗(研究开始时一次由 IUI 联合卵巢刺激和另一个由体外授精而未被确认的怀孕)。在排除所有方案外的治疗中,CLBR 为在IUI 组中的 83 名妇女中22 例 (27%) 活产,在 EM 组的 88 名妇女中 6 名 (7%) 活产(RR= 3.89,95% 可信区间1.66-9.11;p=0.002)。
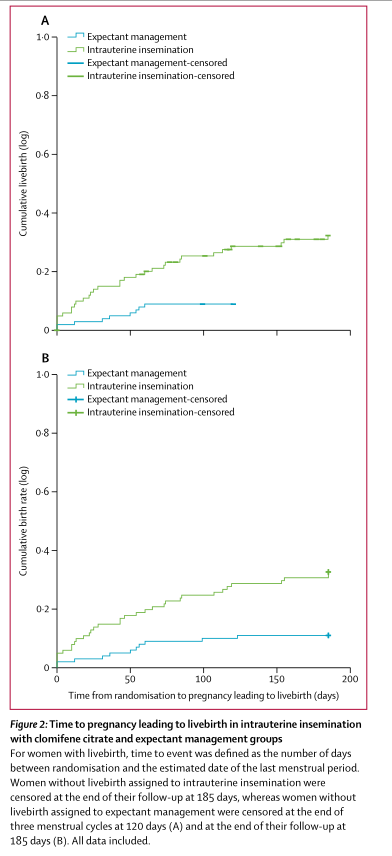
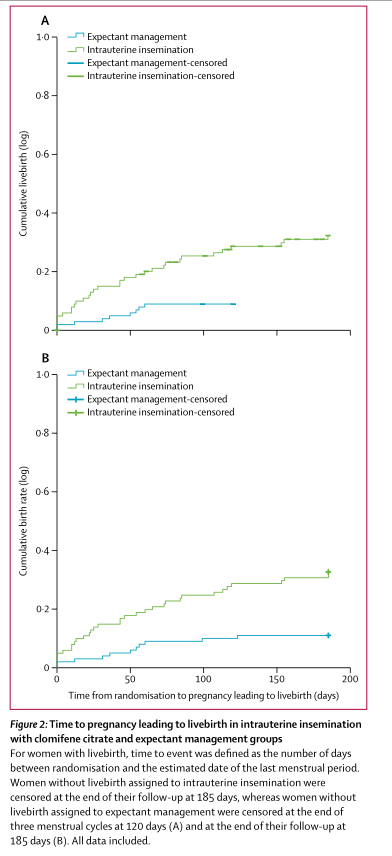
图2克罗米芬宫腔内人工授精组与期待治疗组导致活产的妊娠时间。
Kaplan-Meier 分析表明与 EM 相比,卵巢刺激 IUI 相关的活产率增加(对数秩 [Mantel-Cox]χ²检验 =12.247;df=1; p>0.0001)。
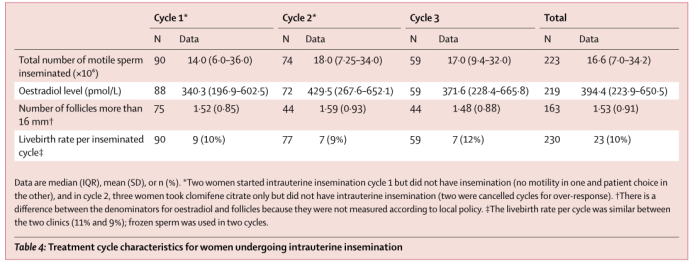
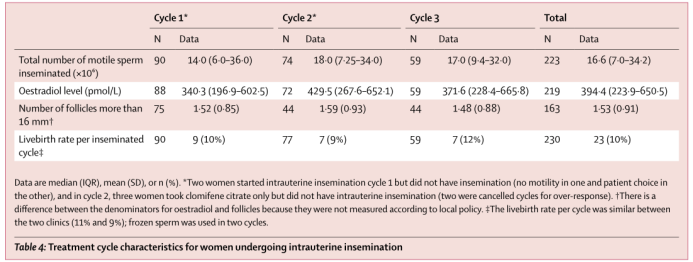
表4接受宫腔内人工授精的妇女的治疗周期特点。数据为中位数(IQR)、平均数(标准差)或n (%)。*2名妇女开始了子宫内人工授精周期1,但没有进行人工授精(1名妇女没有活动能力,另1名妇女被进行了患者选择),在周期2中,三名妇女仅服用了枸橼酸氯米芬,但没有进行子宫内人工授精(两名妇女因过度反应而取消了周期)。†雌二醇和卵泡的测量分母有所不同,因为它们不是根据当地政策测量的。‡两个诊所之间每个周期的活产率相似(11%和9%);冷冻精子用于两个周期。
在两个参与的诊所中共完成了225个IUI周期,92名妇女中有90名(98%)至少接受了一个周期。225个周期中的180个(80%)在一个诊所完成。两个诊所每个周期的活产率相似(一个诊所180个周期的活产率为19例[11%],另一个诊所45个周期的活产率为4例[9%])。
总结:本研究为一项实用、开放、随机、对照、双中心试验,旨在探讨对不明原因不孕且未来12个月内自然受孕预测评分不理想(< 30%)的妇女,比较3个周期IUI联合卵巢刺激(口服枸橼酸氯米芬或来曲唑)与3个周期EM的有效性。结果显示,在这项随机对照试验中,研究结果表明在不明原因不孕和自然受孕预后不良的妇女中,三个周期的IUI卵巢刺激与三个周期的EM相比,CLBR改善了三倍;一个周期的IUI卵巢刺激与三个周期的EM有相似的活产结局;三个周期的IUI卵巢刺激也优于一个周期的IVF-SET。两组双胞胎出生,均在IUI卵巢刺激组(多胎妊娠率6%)。从而验证了研究假设IUI卵巢刺激组的活产率比EM组更高。本研究可以被不明原因不孕的夫妇和他们的生殖科医生在决定用IUI治疗时参考,预测计算器可免费获得,认为IUI可以作为不明原因不孕夫妇的一线治疗。
5、文献点评
优劣势
不足之处:1.本研究使用报告临床试验的推荐方法-意向性治疗分析,在IUI卵巢刺激组中,周期间妊娠的机会增加,可能会高估IUI卵巢刺激的益处,可能会为试验结果带来偏倚。2.本研究IUI组卵巢刺激使用简单的枸橼酸氯米芬方案,然而目前没有足够的证据证明常规使用IUI进行卵巢刺激,该方案缺点主要是多胎妊娠频率高,可能会影响本研究主要结局的可信度。3.本研究IUI卵巢刺激组的5名妇女和EM组的1名妇女在研究开始时有未被确认的怀孕。除非随机化仅在月经周期的前几天进行,否则这是不可避免的,这会为试验结果带来偏倚。4.安排连续的IUI周期并导致5名妇女在IUI卵巢刺激之前或之间自然受孕是比较难实现的。
创新性:本研究为一项实用、开放、随机、对照、双中心试验,旨在探讨对不明原因不孕且未来12个月内自然受孕预测评分不理想(< 30%)的妇女,比较3个周期IUI联合卵巢刺激(口服枸橼酸氯米芬或来曲唑)与3个周期EM的有效性。1.纳入EM组是本研究的优势,三个周期后EM组的CLBR为9%(意向性治疗),该值接近功效计算中的8%估计值,并且类似于英国IUI和EM试验中EM组6个月后的活产率(193名妇女中有32名[17%]活产婴儿)。2.本研究纳入患有多囊卵巢综合征和轻度子宫内膜异位症的妇女或年龄高达40岁的妇女,虽然会降低研究结果,但是却可以反映了无法明确解释其延迟怀孕和寻求生育治疗的妇女的多样性,这也是其他研究者所忽视的问题。3. 根据NICE的建议,即诊所不应提供IUI,而应考虑将IVF作为持续时间超过2年的不明原因不孕症的一线治疗,很少有诊所注意到NICE指南且临床上缺乏对IUI与EM相比的随机对照试验,而本研究正是这样一个随机对照试验,可以说是填补了临床研究的空缺。4. 本研究进行了意向性治疗分析,在意向治疗人群中分析了所有预先指定的结果,在意向治疗和符合方案人群中分析了活产儿;还做了事后敏感性分析,保证了试验数据方案得出结果的全面性。
研究意义(对临床上的指导):本研究可以被不明原因不孕的夫妇和他们的生殖科医生在决定用IUI治疗时参考,预测计算器可免费获得。从而需要重新考虑NICE的建议,即诊所不应提供IUI,而应考虑将IVF作为持续时间超过2年的不明原因不孕症的一线治疗。对于不明原因不孕和预测评分不佳的夫妇,IUI联合卵巢刺激可以作为一种安全且经济的一线策略。
临床思路启发:本研究为一项实用、开放、随机、对照、双中心试验,其研究周期较长,成本并不高昂,研究方案在临床上可以做到,对于普通研究者可以借鉴以下几点:1.可以收集医院内或卫生系统等相关的病人数据,进行回顾性研究。2.可以增加试验样本量,进行类似的大样本临床试验。3.运用相对应的统计分析方法,通过不同的意向治疗和符合方案分析活产。4.可以针对之前研究中存在的问题,进一步严谨进行试验设计,采用新的统计,分析,建模方式进行处理,以期得到不同的研究结论或进一步丰富现有的研究结论。5.目前也有相关研究,比如作者提到有一项比较三个周期IVF-SET和六个周期IUI与促性腺激素的随机对照试验报告了12个月后相似的CLBRs(52%vs47%有意治疗),可以利用中心研究数据重新设置对照组与试验组,甚至可以进行设置多组进行组间比较,研究者可以结合这些相关研究进行综述分析,系统评价或者Meta分析,以期获得更确切的研究结果和不同的证据。
后续研究空间:目前很少有关于IUI的研究考虑IUI如何提高生育率的问题,研究者认为其有效性来自于卵巢刺激导致一个以上卵泡的综合效应,以及在接近可能排卵的时间将准备好的精子放入子宫,后续可以深化研究卵泡效应机制,考虑使用除氯米芬以外的促排卵药物进行卵巢刺激,甚至可以思考精子宫内放置的作用,包括宫颈还是宫腔内放置精子。
二、文献翻译
1、摘要
Background Women with unexplained infertility are often offered intrauterine insemination (IUI) with ovarian stimulation as an alternative to in-vitro fertilisation (IVF). However, little evidence exists that IUI is an effective treatment. In 2013, the UK National Institute for Health and Care Excellence recommended that IUI should not be routinely offered for couples with unexplained infertility.
背景:不明原因不孕的妇女通常接受卵巢刺激子宫内人工授精(IUI)作为体外受精(IVF)的替代方案。然而,几乎没有证据表明IUI是一种有效的治疗方法。2013年,英国国家健康和护理卓越研究所建议,IUI不应作为不明原因不孕夫妇的常规选择。
Methods For this pragmatic, open-label, randomised, controlled, two-centre study, we enrolled women attending two fertility clinics in New Zealand with unexplained infertility and an unfavourable prognosis of natural conception. Participants were randomly assigned (1:1) using a computer-generated randomisation sequence, prepared by an independent statistician, to either three cycles of IUI with ovarian stimulation (with either oral clomifene citrate [50–150 mg, days 2–6] or oral letrozole [2·5–7·5 mg, days 2–6], with choice of ovarian stimulation made by the clinic) or three cycles of expectant management (couples advised to be sexually active around the likely time of ovulation and provided with a diary to record the first day of each menstrual cycle and dates of sexual activity) in blocks of four, six, and ten, without stratification. The participating couple and the clinicians were informed of treatment allocation. The primary outcome was cumulative livebirth rate in the intention-to-treat population. The safety analyses were done in the intention-to-treat population. This study was prospectively registered with the Australian and New Zealand Clinical Trials Register, number ACTRN12612001025820.
方法:在这项实用、开放、随机、对照、双中心的研究中,我们招募了在新西兰两个生育诊所就诊的不明原因不孕且自然受孕预后不良的妇女。受试者被随机分配(1:1)接受三个周期的IUI卵巢刺激(口服枸橼酸氯米芬[50-150mg,第2-6天]或口服来曲唑[2.5-7.5mg,第2-6天],卵巢刺激由诊所选择)或三个周期的期待治疗(建议夫妇在可能的排卵时间进行性活动,并提供日记记录每个月经周期的第一天和性活动的日期)参与的夫妇和临床医生被告知治疗分配。研究的主要结局是意向性治疗人群中的累积活产率。安全性分析在意向性治疗人群中进行。该研究已在澳大利亚和新西兰临床试验注册中心注册,注册号为ACTRN12612001025820。
Findings Between March 12, 2013, and May 12, 2016, we randomly assigned 101 women to IUI with ovarian stimulation and 100 to expectant management, all of whom were included in the primary efficacy analysis and safety analyses. Women assigned to IUI had a higher cumulative livebirth rate than women assigned to expectant management (31 [31%] livebirths among 101 women vs nine [9%] livebirths among 100 women; risk ratio [RR] 3.41, 95% CI 1.71–6.79; p=0.0003). Of 31 livebirths in the IUI group, 23 resulted from IUI cycles and eight were conceived without assistance before or between IUI cycles. Of nine livebirths in the expectant management group, one patient was pregnant from IUI with ovarian stimulation at study entry and one had received off-protocol treatment (IVF). Two sets of twins were born, both in the IUI group (one from a cancelled cycle for over-response).
研究结果:在2013年3月12日至2016年5月12日期间,我们随机将101名妇女分配到IUI进行卵巢刺激,100名妇女分配到期待疗法,所有这些妇女都包括在主要疗效分析和安全性分析中。被分配到IUI的妇女比被分配到期待治疗的妇女有更高的累积活产率(每101名妇女中有31名[31%]活产率,而每100名妇女中有9名[9%]活产率;风险比[RR] 3.41,95%可信区间1.71–6.79;p=0.0003)。在IUI组的31例活产中,23例来自IUI周期,8例是在IUI周期之前或之间在没有辅助的情况下受孕的。在期待治疗组的9例活产儿中,1例来自IUI,研究开始时接受了卵巢刺激,1例接受了方案外治疗(IVF)。两组双胞胎都是在IUI组(一组来自因过度反应而取消的周期)。
Interpretation IUI with ovarian stimulation is a safe and effective treatment for women with unexplained infertility and an unfavourable prognosis for natural conception.
解释:对于不明原因不孕和自然受孕预后不良的妇女,IUI联合卵巢刺激是一种安全有效的治疗方法。
Funding Auckland Medical Research Foundation, Evelyn Bond Fund of Auckland District Health Board, Mercia Barnes Trust of Royal Australian and New Zealand College of Obstetricians and Gynaecologists, Maurice and Phyllis Paykel Trust, and The Nurture Foundation for Reproductive Research.
资助资金:奥克兰医学研究基金会,奥克兰地区卫生局Evelyn Bond基金,澳大利亚和新西兰皇家妇产科学院Mercia Barnes信托基金,Maurice和Phyllis Paykel信托基金以及生殖研究培育基金会。
2、Introduction
前言
Intrauterine insemination (IUI) is widely used in the USA, the UK, and Europe as a low-cost, less-invasive alternative to in-vitro fertilisation (IVF) for couples with unexplained infertility. IUI of sperm suspension is done at the estimated time of ovulation in a natural cycle or after ovarian stimulation.译【子宫内人工授精(IUI)在美国、英国和欧洲广泛使用,作为不明原因不孕夫妇体外受精(IVF)的一种低成本、侵入性较小的替代方法。在自然周期的预计排卵时间或卵巢刺激后进行IUI精子悬浮。】Several randomised controlled trials of IUI have been done, but only two have considered the question of whether IUI is superior to expectant management (EM),
and neither have provided evidence of effectiveness. One trial of IUI versus EM did not include ovarian stimulation and did not report evidence of benefit after 6 months, with livebirth rates of 23% versus 17%. In the other trial, women with intermediate prognosis for natural conception had six cycles of IUI with ovarian stimulation versus EM and the ongoing pregnancy rate was 23% versus 27%.译【已经进行了几项关于IUI的随机对照试验,但是只有两项考虑了IUI是否优于期待疗法(EM)的问题,并且都没有提供有效性的证据。一项IUI与EM的试验不包括卵巢刺激,并且没有报告6个月后受益的证据,活产率为23%和17%。在另一项试验中,6名自然受孕预后中等的妇女接受了6个周期的IUI卵巢刺激和EM治疗,持续妊娠率分别为23%和27%。】The UK National Institute for Health and Care Excellence (NICE) recommended in 2013 that intrauterine insemination, with or without ovarian stimul-
ation, should not be routinely offered to couples with unexplained infertility and that IVF could be considered after 2 years of EM. However, a 2015 survey of UK fer tility clinicians reported that 96% continued to offer IUI.译【英国国家健康与护理卓越研究所(NICE)在2013年建议,无论是否有卵巢刺激,都不应常规向不明原因不孕的夫妇提供子宫内受精,并且可以在期待治疗2年后考虑IVF。然而,2015年对英国不孕临床医生的调查报告称,给96%的人继续提供IUI.】We aimed to compare the effectiveness of three cycles of IUI with ovarian stimulation (oral clomifene citrate or letrozole) versus three cycles of EM in women with unexplained infertility and an unfavourable prediction score for natural conception (<30%) in the next 12 months. We wished to test the hypothesis that livebirth rates would be higher in the IUI with ovarian stimulation group.译【我们旨在对不明原因不孕且未来12个月内自然受孕预测评分不理想(< 30%)的妇女,比较3个周期IUI联合卵巢刺激(口服枸橼酸氯米芬或来曲唑)与3个周期EM的有效性。我们希望验证IUI卵巢刺激组的活产率更高的假设。】
3、Methods
方法
Study design and participants
研究设计和参与者
The Uterine Insemination (TUI) study was a pragmatic, open-label, randomised, controlled, two-centre study of women with unexplained infertility and an unfavourable
prognosis for natural conception. 译【子宫授精(TUI)研究是一项实用、开放、随机、对照、双中心的研究,研究对象为不明原因不孕且自然受孕预后不良的女性。】The New Zealand Ministry of Health Northern B Regional Ethics Committee approved the study protocol (12/NTB/41/AM03). Women attending fertility clinics (Fertility Plus, Auckland District Health Board and Repromed Auckland) in Auckland, New Zealand, were invited to participate. A written patient information sheet was given to all eligible
women. All participants provided written informed consent before randomisation. We included women younger than 42 years with body-mass index of less than 35 kg/m² and
unexplained infertility, which was defined as normal ovulation (or normal with ovarian stimulation), bilateral patent fallopian tubes as determined by laparoscopy or hysterosalpingography, normal semen analysis (progressive motility of ≥32% and concentration of ≥15 million per mL), and a prediction score of natural conception leading to livebirth in the next year of less than 30%. 译【我们纳入了年龄小于42岁、体重指数小于35 kg/m、不明原因不孕(定义为正常排卵(或卵巢刺激正常)、通过腹腔镜或子宫输卵管造影术确定双侧输卵管通畅、精液分析正常(进行性活动率≥32%、浓度≥1500万/mL)、自然受孕导致下一年活产的预测分数小于30%)的女性。】We used the validated Hunault prediction model for natural conception, which includes age, length of infertility, any previous pregnancies, source of referral, and sperm motility. 译【我们使用了经过验证的Hunault自然受孕预测模型,包括年龄、不孕时间、既往妊娠史、转诊来源和精子活力。】We included women with mild endometriosis (diagnosed by laparoscopy), polycystic ovarian syndrome according to the Rotterdam criteria (providing ovulation was confirmed with or without ovarian stimulation for at least six cycles),and previous IUI or IVF cycles, but we excluded those requiring donor sperm. 译【我们纳入了轻度子宫内膜异位症(经腹腔镜检查确诊)、多囊卵巢综合征(根据鹿特丹标准(假设至少6个周期内有或无卵巢刺激证实排卵)、以及既往IUI或IVF周期的妇女,但我们排除了需要供体精子的妇女。】All women had screening tests before entry in the study: cervical smear less than 3 years before enrolment, high vaginal swabs, viral testing, and immunity against rubella.
Randomisation and masking
随机化和隐蔽
We used a computer-generated randomisation sequence, prepared by an independent statistician, to randomly assign women (1:1) to three cycles of IUI with ovarian
stimulation or three cycles of EM in blocks of four, six, and ten, without stratification.译【我们使用了一个由独立统计学家准备的计算机生成的随机序列,将妇女(1:1)随机分配到3个周期的IUI卵巢刺激或3个周期的EM,每组4个、6个和10个,不分层。】 Allocations were concealed in sequentially numbered, sealed, opaque envelopes, which were opened by the study coordinator at the University of Auckland research department after verification of the inclusion criteria and obtaining written informed consent from each participant. The participating couple and the clinicians were informed of treatment allocation.
Procedures
规程
Both clinics used the same study protocol. In the IUI with ovarian stimulation group, women received oral clomifene citrate (Merck Serono; 50–150 mg, days 2–6) or oral letrozole (Douglas Pharma ceuticals; 2.5–7.5 mg, days 2–6) for ovarian stimulation according to the patient response. 译【两家诊所使用相同的研究方案。在IUI卵巢刺激组,妇女接受口服枸橼酸氯米芬(默克雪兰诺;50–150毫克,第2–6天)或口服来曲唑(道格拉斯制药公司;2.5-7.5毫克,第2-6天)根据患者反应进行卵巢刺激。】The choice of ovarian stimulation was made by the clinic. When one to three follicles were present, IUI was performed by injecting the prepared sample of 0.5 mL sperm into the uterus. Oestradiol and luteinising hormone were measured on day 7 .译【当有1-3个卵泡时,将制备好的0.5ml精子注射入子宫进行IUI。在第7天测量雌二醇和黄体生成素。】 Serial ultrasounds started when oestradiol was higher than 400 pmol/L in the first cycle and if clinically indicated on subsequent cycles. 译【在第一个周期中,当雌二醇高于400 pmol/L时,如果在随后的周期中有临床指征,开始进行系列超声检查。】Daily luteinising hormone tracking started when the leading follicle was 14 mm or larger in diameter or when oestradiol reached 400 pmol/L. When one to three follicles were present, IUI was performed approximately 24 h after the luteinising hormone surge or 36 h after a human chorionic gonadotropin trigger injection. 译【当第一个卵泡直径大于或等于14 mm或雌二醇达到400 pmol/L时,开始每日追踪黄体生成素。当出现1-3个卵泡时,在黄体生成素高峰后约24小时或人绒毛膜促性腺激素触发注射后36小时进行IUI。】Ultrasound was generally not used in the second or third cycle unless the oestradiol level was 2000 pmol/L or higher.译【 除非雌二醇水平为2000 pmol/L或更高,否则在第二或第三周期中通常不使用超声。】Letrozole cycles were monitored with both oestradiol levels and ultrasound.
The semen sample was prepared using density gradients of 45% and 90%, and following centrifugation the sample was washed in 3 mL of culture media and resuspended in 0·5 mL of culture media. A TomCat catheter (Santesel, Turkey) was used for a single insemination. The prepared sperm sample of 0·5 mL was injected into the uterus. Luteal support was not routinely given. If 7 days after insemination, the progesterone level was less than 20 pmol/L, utrogestan vaginal pessaries 200 mg three times a day were started. Serum β-human chorionic gonadotropin was measured 14 days after the insemination.译【黄体支持不是常规给予的。如果在授精后7天,孕酮水平低于20 pmol/L,则开始每天三次200 mg的黄体酮栓剂阴塞。授精后14天测定血清β-人绒毛膜促性腺激素水平。】
Cycles were cancelled if there was no response (no rise in the oestradiol or development of follicles) or if there were more than three follicles (in which case women were requested to avoid unprotected intercourse). The cancelled cycle was replaced by a further cycle with appropriate dose adjustment.译【如果没有反应(雌二醇没有上升或卵泡没有发育)或如果有三个以上的卵泡(在这种情况下,要求妇女避免无保护的性交),则周期被取消。被取消的周期被另一个具有适当剂量调整的周期所替代。】
No major protocol changes were made to the inclusion criteria or the treatment interventions during the study. However, consecutive scheduling of IUI with ovarian stimulation cycles was not always possible because of cancellations, scheduling difficulties, and early pregnancy losses. 译【然而,由于取消、时间安排困难和早期妊娠损失,连续安排IUI和卵巢刺激周期并不总是可能的。】After discussions with the Data Safety Monitoring Committee in early 2014 it was agreed that livebirths would only be included if three IUI cycles were completed within 6 months (185 days) from the date of randomisation.译【在2014年初与数据安全监测委员会讨论后,双方同意只有在随机分组之日起6个月(185天)内完成三个IUI周期的情况下,才纳入活产儿。】Exceptions would be made in the case of miscarriage, when women were allowed recovery time and then time to complete their allocated number of IUI cycles. Natural conceptions were included if they occurred before all three IUI cycles were completed. If an ectopic pregnancy occurred then no further IUI cycles were done.译【流产的情况例外,妇女有恢复时间,然后有时间完成分配给她们的IUI周期数。如果它们发生在所有三个IUI周期完成之前的自然受孕包括在内。如果发生宫外孕,则不再进行IUI周期。】
Couples assigned to EM were followed up for three cycles. They were advised to be sexually active around the likely time of ovulation and were provided with a diary to record the first day of each menstrual cycle and dates of sexual activity. Women in the EM group who had anovulatory polycystic ovary syndrome continued with their ovulation induction.译【被分配到EM组的夫妇接受了三个周期的随访。他们被建议在可能的排卵时间进行性活动,并被提供一本日记来记录每个月经周期的第一天和性活动的日期。EM组中患有无排卵性多囊卵巢综合征的妇女继续接受促排卵治疗。】
We collected the following data for all couples: age, body-mass index, smoking (ever), ethnicity, previous livebirths, previous IVF or IUI cycles, duration of infertility, diagnosis of anovulatory polycystic ovary syndrome and mild endometriosis, anti-Müllerian hormone level, sperm count and motility, and Hunault prediction score for natural conception over the next 12 months.译【我们收集了所有夫妇的以下数据:年龄、体重指数、是否吸烟、种族、既往活产、既往IVF或IUI周期、不孕持续时间、无排卵性多囊卵巢综合征和轻度子宫内膜异位症的诊断、抗苗勒管激素水平、精子计数和活动力以及未来12个月自然受孕的Hunault预测评分。】 For couples randomly assigned to the IUI with ovarian stimulation group, additional data were collected regarding the type of stimulation protocol (clomifene or letrozole); day 12 oestradiol level; number of follicles more than 16 mm in diameter on day 12; use of ovarian trigger (if follicle ≥18 mm in diameter and no luteinising hormone rise detected); luteal phase support; fresh or frozen sperm; and total motile sperm inseminated.译【对于随机分配到IUI卵巢刺激组的夫妇,收集了关于刺激方案类型(克罗米芬或来曲唑)的其他数据;第12天雌二醇水平;第12天直径大于16 mm的卵泡数;使用卵巢触发剂(如果卵泡直径≥18 mm且未检测到黄体生成素升高);黄体期支持;新鲜或冷冻精子;和受精的活动精子总数。】
Pregnancy outcomes and treatment details were collected either from the electronic health record using the National Health Index number or from the fertility clinic records. The study coordinator entered the data into the database at the University of Auckland. The study clinicians were not formally informed of pregnancy outcomes by the study coordinator, but masking of study clinicians to the allocation or pregnancy outcomes was not always possible because of their clinical involvement. The study records were kept confidential and secure.
Outcomes
结局
The primary outcome was livebirth rate after three cycles of treatment and was reported as cumulative livebirth rate (CLBR) in the intention-to-treat population. 译【主要转归是三个治疗周期后的活产率,并报告为意向性治疗人群中的累积活产率(CLBR)。】Secondary outcomes were clinical pregnancy, ectopic pregnancy, miscarriage, multiple pregnancy, ovarian hyper stimulation syndrome, time to pregnancy leading to a livebirth, and birthweight. 译【次要转归是临床妊娠、异位妊娠、流产、多胎妊娠、卵巢过度刺激综合征、导致活产的妊娠时间和出生体重。】Livebirth, clinical pregnancy, and miscarriage were defined using WHO criteria.14,15 Women reported pregnancy directly to the study coordinator, whereas cycle treatment and other clinical outcomes such as livebirth were obtained from electronic medical records using the National Health Index number.
Statistical analysis
统计学分析
We calculated that a sample of 80 women in each group would provide 80% power at a significance level of 0.05 (one-sided test) to detect a difference of 14% in CLBR. 译【我们计算出,每组80名女性的样本在显著性水平为0.05(单侧检验)时将提供80%的功效,以检测CLBR 14%的差异。】We assumed a CLBR of 22% for IUI with ovarian stimulation and 8% for EM on the basis of recent data from one of the participating fertility clinics. The final target was 100 in each group because the natural conception rate in the IUI with ovarian stimulation group was higher than predicted. 译【根据一个参与的生育诊所最近的数据,我们假设卵巢刺激IUI的CLBR为22%,子宫内膜异位症为8%。每组的最终目标是100,因为IUI卵巢刺激组的自然受孕率高于预期。】We did not stratify by study centre because we did not anticipate demographic or clinical differences between women recruited at the two centres, which are both in the same region.译【我们没有按研究中心进行分层,因为我们没有预料到在同一地区的两个中心招募的妇女之间的人口统计学或临床差异。】
We did the following preplanned analyses: intention-to-treat analysis of all randomly assigned women, post-randomisation intention-to-treat analysis excluding women who were ineligible (such as with a prediction score breach [≥30%] or pregnant at study entry), and per-protocol analysis excluding women who were ineligible and women with protocol violations (defined in the EM group as having any fertility treatment during the three cycles from randomisation and in the IUI with ovarian stimulation group as having an IVF cycle or being pregnant before or between cycles). 译【我们进行了以下预先计划的分析:对所有随机分配的妇女进行意向性治疗分析,排除不合格妇女的随机化后意向性治疗分析(如预测评分违反[≥30%]或在研究开始时怀孕),以及排除不合格妇女和违反方案的妇女(EM组定义为在随机分配后的三个周期内进行任何生育治疗,IUI卵巢刺激组定义为进行IVF周期或在周期前或周期间怀孕)。】All prespecified outcomes were analysed in the intention-to-treat population and livebirths were analysed in the intention-to-treat and per-protocol populations. We also did post-hoc sensitivity analyses; first, excluding from the per-protocol analysis women who only had clomifene citrate in the IUI group (strict per protocol), and second, examining differing durations of follow-up (120 days and 185 days from randomisation) to assess the possible effect of treatment delays in the IUI with ovarian stimulation group.译【我们还做了事后敏感性分析;首先,从方案分析中排除IUI组(严格按照方案)中仅使用枸橼酸氯米芬的妇女,其次,检查不同的随访持续时间(从随机分组开始的120天和185天)以评估卵巢刺激IUI组中治疗延迟的可能影响。】
For dichotomous variables, we calculated risk ratios (RR) with 95% CIs and tested significance using the χ² test. For continuous variables, we used the Student’s t test or a Kruskal-Wallis test. We plotted Kaplan-Meier curves to examine any differences in time to livebirth between the IUI with ovarian stimulation and EM groups. We compared these curves with a log-rank (Mantel-Cox) test. Analyses were done using IBM SPSS Statistics Version 23. An independent Data Safety Monitoring Committee reviewed the data collection and advised that there were no safety concerns.译【对于二分变量,我们用95% CIs计算风险比(RR ),并用χ2检验检验显著性。对于连续变量,我们使用学生的t检验或Kruskal-Wallis检验。我们绘制了Kaplan-Meier曲线来检测卵巢刺激IUI组和EM组之间的存活时间差异。我们用对数秩(Mantel-Cox)检验比较了这些曲线。使用IBM SPSS Statistics第23版进行分析。】
This study was prospectively registered with the Australian and New Zealand Clinical Trials Register, number ACTRN12612001025820.
Role of the funding source
资金来源者的角色
The funders of the study had no role in study design, data collection, data analysis, data interpretation, or writing of the report. The corresponding author had full access to all the data in the study and had final responsibility for the decision to submit for publication.
4、Results
结果
We screened 473 women for eligibility. Of 341 eligible women invited to take part, 140 declined and 201 were randomly assigned to a group between March 12, 2013, and May 12, 2016: 101 to IUI with ovarian stimulation and 100 to EM (figure 1).译【我们对473名女性进行了资格审查。在341名受邀参加的合格女性中,140名拒绝,201名在2013年3月12日至2016年5月12日之间被随机分配到一个组:101名妇女研究方案是IUI接受卵巢刺激,100名妇女研究方案是EM(图1)。】 The only significant difference between women agreeing or declining to participate was that women who declined had a shorter duration of infertility (median 24 months vs 44 months; p=0.03) and were more likely to be parous (38 [27%] of 142 vs 25 [12%] of 201; p=0.0009). No data were missing for any of the pregnancy, livebirth, or neonatal outcomes. Baseline characteristics were similar between the two groups (table 1).
译【同意或拒绝参与的妇女之间唯一的显著差异是拒绝参与的妇女不孕症持续时间较短(中位数24个月对44个月;p = 0.03)并且更可能是经产的(142人中的38人[27%]对201人中的25人[12%];p=0.0009)。没有遗漏任何妊娠、活产或新生儿结局的数据。两组之间的基线特征相似(表1)。】
The IUI group had a higher CLBR than the EM group (31 [31%] livebirths among 101 women vs nine [9%] livebirths among 100 women; RR 3.41, 95% CI 1.71–6.79; p=0.0003; tables 2, 3). 译【IUI组的CLBR高于EM组(每101名妇女中有31名[31%]活产儿,而每100名妇女中有9名[9%]活产儿;相对危险度为3.41,95%可信区间为1.71–6.79;p = 0.0003表2、3)。】Of the 31 livebirths in the IUI group, 23 resulted from IUI cycles, three from unrecognised pregnancies at study entry, and five were conceived before or between IUI cycles. Of the nine livebirths in the EM group, two resulted from off-protocol treatment (one unrecognised pregnancy at study entry resulting from IUI with ovarian stimulation and another resulting from IVF). In an analysis excluding all protocol violations, the CLBR was 22 (27%) livebirths among 83 women in the IUI group and six (7%) livebirths among 88 women in the EM group (RR 3.89, 1.66–9.11; p=0.002). These results suggest that five women would need to be treated with three IUI cycles to achieve one additional livebirth (95% CI 3–9; using intention-to-treat data). 译【这些结果表明,5名妇女需要接受3个IUI周期的治疗才能获得一个额外的活产儿(95%可信区间3–9;使用意向性治疗数据)。】 Of the six women with anovulatory polycystic ovary syndrome in the EM group, all continued with clomifene citrate and none conceived, and of four women with anovulatory polycystic ovary syndrome in the IUI group, one conceived.
Kaplan-Meier analysis suggested an increased chance of a livebirth associated with IUI with ovarian stimulation compared with EM (log-rank [Mantel-Cox] test χ²=12.247; df=1; p>0·0001; figure 2).译【Kaplan-Meier分析表明,与EM相比,卵巢刺激IUI相关的活产机会增加(log-rank [Mantel-Cox]检验χ²= 12.247;df = 1;p > 0.0001图2)。】
We found no significant differences between the groups in rates of pregnancy-related adverse events. In the IUI group, two sets of twins were born (one following cancelled cycle for over-response) and four ectopic pregnancies occurred (two from unrecognised pregnancies at study entry and two following IUI cycles); 译【我们发现两组之间妊娠相关不良事件的发生率没有显著差异。在IUI组中,出生了两组双胞胎(一组是在因过度反应而取消周期后出生的)和发生了四次异位妊娠(两次是在研究开始时未确认的妊娠,两次是在IUI周期后发生的);miscarriages occurred in six (16%) of 37 clinical pregnancies. In the EM group, one (9%) miscarriage occurred among the 11 clinical pregnancies.
Mean birthweight for the 33 babies in the IUI group was 3166 g (SD 638), including two sets of twins born at 36 weeks and 38 weeks gestation, respectively. Mean birthweight for the nine babies in the EM group was 3470 g (SD 654; p=0.21 for difference between groups). 译【IUI组33名婴儿的平均出生体重为3166克(SD 638),包括分别在妊娠36周和38周出生的两组双胞胎。EM组9名婴儿的平均出生体重为3470克(SD 654组间差异p = 0.21)。】 In the IUI group, one baby was born preterm at 31 weeks gestation following placental abruption and another was born at term with a known tetralogy of Fallot; both required specialist care and were healthy at follow-up. In the EM group, one stillbirth occurred at 20 weeks gestation as a result of pregnancy following off-protocol treatment with IUI with ovarian stimulation in the third cycle. All other babies were born at term and considered healthy.
A total of 225 IUI cycles were completed at the two participating clinics (table 4), and 90 (98%) of 92 women had at least one cycle. 180 (80%) of 225 cycles were completed at one clinic. The livebirth rate per cycle was similar between the two clinics (19 [11%] births from 180 cycles at one clinic vs four [9%] births from 45 cycles at the other). 译【在两个参与的诊所中共完成了225个IUI周期(表4),92名妇女中有90名(98%)至少接受了一个周期。225个周期中的180个(80%)在一个诊所完成。两个诊所每个周期的活产率相似(一个诊所180个周期的活产率为19例[11%],另一个诊所45个周期的活产率为4例[9%])。】All IUI cycles with a livebirth were commenced within 6 months of randomisation, except for one woman whose second cycle was delayed due to miscarriage. No cases of ovarian hyperstimulation occurred. With the exception of one participant in cycles 2 and 3, all cycles used fresh sperm. Only seven women received letrozole rather than clomifene citrate.
A trigger was used in 34 (15%) of 225 cycles and luteal support in five (22%) of 225 cycles. Four pregnancies leading to livebirth occurred in the women who had a trigger. No pregnancies occurred in the women who received luteal phase support. 34 (15%) of 225 cycles (over the three cycles) were cancelled: 17 were for over-response, five for under-response, and four by patient choice (in eight cases, no reason was provided). In the EM group, 72 (72%) women returned their diaries and reported on dates of sexual intercourse between day 10 and 18 of the cycle. The mean frequency of sex was 3·1 (SD 1·3) for cycle 1 (n=72), 3·5 (1·7) for cycle 2 (n=71), and 3·6 (1·5) for cycle 3 (n=67). 译【在EM组中,72名(72%)妇女归还了她们的日记,并报告了在月经周期的第10天和第18天之间的性交日期。第1周期(n=72),第2周期(n=71)和第3周期(n=67)的平均性生活频率分别为3.1 (SD 1.3),3.5 (1.7)和3.6 (1.5)。】One or two women in each cycle had no sexual activity recorded.
5、Discussion
讨论
In this randomised controlled trial, we have reported that, in women with unexplained infertility and an unfavourable prognosis for natural conception, three cycles of IUI with ovarian stimulation were associated with a three-fold improved CLBR compared with three cycles of EM. 译【在这项随机对照试验中,我们报道了在不明原因不孕和自然受孕预后不良的妇女中,三个周期的IUI卵巢刺激与三个周期的EM相比,CLBR改善了三倍。Two sets of twins were born, both in the IUI with ovarian stimulation group (6% multiple pregnancy rate).译【两组双胞胎出生,均在IUI卵巢刺激组(多胎妊娠率6%)。】
Although an intention-to-treat analysis is the recommended approach for reporting clinical trials, concerns might exist that the intention-to-treat analysis in this study would overestimate the benefits of IUI with ovarian stimulation because of the increased opportunity for between-cycle pregnancies in the IUI with ovarian stimulation group. 译【尽管意向性治疗分析是报告临床试验的推荐方法,但可能存在这样的担忧,即本研究中的意向性治疗分析会高估IUI卵巢刺激的益处,因为在IUI卵巢刺激组中,周期间妊娠的机会增加。】A per-protocol analysis might therefore be more appropriate. Alternatively, we could argue that the more reliable outcome is the number of pregnancies leading to livebirth using the full dataset (intention-to-treat) up to 120 days from randomisation because the data are complete, data collection was planned, there were no post-randomisation exclusions, and the length of follow-up was the same in both groups. 译【或者,我们可以认为更可靠的结果是从随机分组开始到120天使用完整数据集(意向性治疗)导致活产的妊娠数,因为数据是完整的,数据收集是有计划的,没有随机分组后的排除,并且两组的随访时间是相同的。】Although our findings were robust to each of the analyses, we favour the planned intention-to-treat analysis for this pragmatic trial because scheduling consecutive cycles and managing early pregnancy losses are a daily reality of fertility clinics. 译【虽然我们的研究结果对每一项分析都是可靠的,但我们更倾向于对这一实际的试验进行有计划的意向性治疗分析,因为安排连续周期和管理早期妊娠损失是生育诊所的日常写照。】We are also confident that no data were missing for the primary outcome because we were able to check birth records using the National Health Index number.
The inclusion of an EM group was a major strength of our study. The CLBR in the EM group was 9% (intention-to-treat) after three cycles, which might seem low; however, the value is close to the 8% estimate in the power calculation and similar to the livebirth rate (32 [17%] livebirths among 193 women) after 6 months in the EM group in the UK trial of IUI and EM.译【纳入EM组是我们研究的主要优势。三个周期后,EM组的CLBR为9%(意向性治疗),这可能看起来很低;然而,该值接近功效计算中的8%估计值,并且类似于英国IUI和EM试验中EM组6个月后的活产率(193名妇女中有32名[17%]活产婴儿)。】Although only 72% of women in the EM group in our study reported on the frequency of sexual activity, these data provide some indication that women were actively trying to conceive. 译【尽管在我们的研究中EM组只有72%的妇女报告了性活动的频率,但这些数据提供了一些妇女积极尝试怀孕的迹象。】We also note that only five women from the EM group had other fertility treatments.
We used a simple clomifene citrate protocol for ovarian stimulation in most cases. Gonadotropins are the most commonly used stimulation protocol but have disadvantages including a high frequency of multiple pregnancy.译【在大多数情况下,我们使用简单的枸橼酸氯米芬方案进行卵巢刺激。促性腺激素是最常用的刺激方案,但其缺点包括多胎妊娠频率高。】We allowed the clinics to use triggering and luteal phase support if clinically indicated because insufficient evidence exists for routine use of IUI with ovarian stimulation. 译【因为没有足够的证据证明常规使用IUI进行卵巢刺激,如果有临床指征,我们允许诊所使用触发和黄体期支持。】
We acknowledge limitations in both study design and conduct. First, five women in the IUI with ovarian stimulation group and one in the EM group had unrecognised pregnancies at study entry. This is inevitable unless randomisation is only done on the first few days of the menstrual cycle. Second, scheduling the consecutive cycles of IUI proved to be challenging and led to five women conceiving naturally before or between IUI with ovarian stimulation cycles. 译【我们承认研究设计和实施中的局限性。首先,IUI卵巢刺激组的五名妇女和EM组的一名妇女在研究开始时有未被确认的怀孕,除非随机化仅在月经周期的前几天进行,否则这是不可避免的。第二,安排连续的IUI周期被证明是具有挑战性的,并导致五名妇女在IUI卵巢刺激周期之前或之后自然受孕。】This is not uncommon in fertility studies and women might have a “rest” or “take a break” from the treatment for some cycles. Failure to complete the full study protocol is also common among trials of IUI. In the UK trial of IUI, only 19% of women completed six cycles. Some study designs have attempted to overcome these challenges by giving women 12 months to complete six cycles of IUI and by using intention-to-treat analysis including all off-protocol pregnancies. 译【在IUI的英国试验中,只有19%的女性完成了六个周期。一些研究设计试图通过给女性12个月的时间来完成六个周期的IUI,并通过使用包括所有非协议怀孕在内的意向性治疗分析来克服这些挑战。】Third, 8% of women had a higher prediction score than our protocol allowed, in most cases because clinical staff recruiting women overlooked counting early pregnancy loss as a pregnancy. 译【第三,在大多数情况下,因为招募女性的临床工作人员忽略了将早期妊娠损失算作一次妊娠,因此8%的女性预测得分高于我们的研究方案允许值。】 Other breaches included pregnancies in three women who started clomifene citrate but did not have the insemination. These breaches reflect the challenges of doing a pragmatic trial in real-world clinics, and sensitivity analyses excluding these women did not substantially affect our findings. The study protocol also allowed us to include women with a diagnosis of anovulatory polycystic ovary syndrome who had already been treated with ovarian induction over at least six cycles. Less than 5% of women were in this category. 10% of women had a diagnosis of mild endometriosis, but in all cases, they had patent fallopian tubes. Other studies of unexplained infertility have included women with mild endometriosis. 译【研究方案还允许我们纳入诊断为无排卵性多囊卵巢综合征的妇女,她们已经接受了至少6个周期的卵巢诱导治疗。不到5%的女性属于这一类别。10%的女性被诊断为轻度子宫内膜异位症,但在所有病例中,她们都有输卵管通畅。其他不明原因不孕的研究包括轻度子宫内膜异位症妇女。】Some readers might also be concerned that we planned to include women up to 42 years old. The mean age was 34 years and all the women were aged 40 years or younger. We do not consider that the inclusion of women with polycystic ovary syndrome and mild endometriosis or women up to 40 years old detracts from the study results but instead reflects the diversity of women who have no clear explanation for their delay in conceiving and who are seeking fertility treatments.译【一些读者可能也担心我们计划包括42岁以下的妇女。我们纳入的患者平均年龄为34岁,所有妇女都在40岁或以下。我们不认为纳入患有多囊卵巢综合征和轻度子宫内膜异位症的妇女或年龄高达40岁的妇女会降低研究结果,而是反映了无法明确解释其延迟怀孕和寻求生育治疗的妇女的多样性。】
Multiple pregnancy is regarded as an adverse event of fertility treatments. The proportion in our study was 6%. Although this number might seem low compared with the frequency of multiple pregnancy reported following gonadotropins, which can be as high as 22%, the number is similar to frequencies reported in studies of IVF with a single embryo transfer (IVF-SET), which is usually no more than 5%.译【多胎妊娠被视为生育治疗的不良事件。在我们的研究中,这一比例为6%。尽管与促性腺激素治疗后报道的高达22%的多胎妊娠频率相比,这一数值似乎较低,但这一数值与单胚胎移植(IVF-SET)IVF研究中报道的频率相似,通常不超过5%。】With a lower burden of treatment, IUI seems to be preferable to IVF, but if the frequency of multiple pregnancies is shown to be higher with IUI with ovarian stimulation than with IVF-SET , then IVF might be deemed more patient friendly.译【由于治疗负担较低,IUI似乎优于IVF,但如果显示卵巢刺激IUI治疗的多胎妊娠频率高于IVF-SET,则IVF可能被认为对患者更友好。】
Our findings could be considered by couples with unexplained infertility in conjunction with their fertility clinicians, when making decisions about treatment with IUI. The prediction calculator is freely available. Our results seem applicable to other settings because our livebirth rate per IUI with ovarian stimulation cycle was 10%, which is similar to other studies. 译【我们的发现可以给不明原因不孕的夫妇和他们的生育医生在决定用IUI治疗时给出指导意见。预测计算器可免费获得。我们的结果似乎适用于其他情况,因为我们的每IUI卵巢刺激周期的活产率为10%,这与其他研究相似。】We did not do a cost analysis because EM is not associated with any additional costs unless off-protocol treatment occurs. However, cost-effectiveness data from a Dutch randomised controlled trial of IUI with gonadotropins versus IVF-SET took neonatal costs into consideration and reported IUI to be the most cost-effective strategy.译【我们没有进行成本分析,因为EM与任何额外成本无关,除非进行方案外治疗。然而,荷兰一项关于IUI促性腺激素与IVF-SET的随机对照试验的成本效益数据考虑了新生儿成本,并报告IUI是最具成本效益的策略。】
Few studies of IUI have considered the question of how IUI improves fertility. We suggest that its effectiveness derives from the combined effect of ovarian stimulation resulting in more than one follicle, and the placement of prepared sperm into the uterus close to the timing of likely ovulation. 译【很少有关IUI的研究考虑了IUI如何提高生育率的问题。我们认为其有效性来自于卵巢刺激导致一个以上卵泡的综合效应,以及在接近可能排卵的时间将准备好的精子放入子宫。】The use of clomifene for ovarian stimulation is unlikely to be the sole reason that IUI with clomifene is effective because clomifene has not been shown to be superior to unstimulated IUI or EM in ovulatory women. 译【使用氯米芬进行卵巢刺激不太可能是IUI联合氯米芬有效的唯一原因,因为氯米芬并未显示出在排卵期妇女中优于未刺激的IUI或EM。】Laboratory techniques for sperm preparation, such as gradient tests, aim to separate motile sperm from seminal plasma and at the same time remove foreign material that has been reported to inhibit the ability of spermatozoa to fertilise. With regard to the role of the intrauterine placement of sperm, studies comparing intracervical and IUI using donor sperm suggest benefit with IUI using cryopreserved sperm, suggesting that intrauterine placement might have an important role.译【关于精子宫内放置的作用,使用供体精子比较宫颈内放置和IUI放置的研究表明,使用冷冻保存的精子进行IUI是有益的,这表明宫内放置可能具有重要作用。】
Our results offer reliable evidence of a moderate benefit with three cycles of IUI with ovarian stimulation compared with EM. One cycle of IUI with ovarian stimulation had similar livebirth outcomes to three cycles of EM. Our findings after three cycles of IUI with ovarian stimulation also compare favourably with outcomes following one cycle of IVF-SET .译【我们的结果提供了可靠的证据表明,与EM相比,三个周期的IUI卵巢刺激治疗有一定的益处。一个周期的卵巢刺激IUI与三个周期的EM有相似的活产结局。我们在三个周期的卵巢刺激IUI后的发现也优于一个周期的IVF-SET。】A randomised controlled trial comparing three cycles of IVF-SET versus six cycles of IUI with gonadotropins reported similar CLBRs after 12 months (52% vs 47% by intention to treat), with lower health-care costs in the IUI group. 译【一项比较三个周期IVF-SET和六个周期IUI与促性腺激素的随机对照试验报告了12个月后相似的CLBRs对47%有意治疗),IUI组的医疗费用较低。】 The authors stated that there was no reason to abandon IUI as a first-line treatment for couples with unexplained infertility. 译【作者表示,没有理由放弃IUI作为不明原因不孕夫妇的一线治疗。】
The CLBR of 23% following three cycles of IUI with ovarian stimulation in our study is similar to livebirth rates with a single cycle of IVF (fresh transfer only) of 21% for Australia and New Zealand in 2014 and 25% in the UK in 2013. 译【在我们的研究中,三个周期的IUI卵巢刺激后的CLBR为23%,与2014年澳大利亚和新西兰单周期IVF(仅新鲜移植)的活产率21%和2013年英国的25%相似。】Unfortunately, these data are not cumulative because they do not include outcomes from frozen embryo transfers. 译【不幸的是,这些数据不是累积的,因为它们不包括冷冻胚胎移植的结果。】
The question that this study set out to answer was of effectiveness: that is, whether IUI with ovarian stimulation is associated with better outcomes than EM in women with unexplained infertility and an unfavourable prognosis. 译【这项研究要回答的问题是有效性:即对于不明原因不孕和预后不良的妇女,卵巢刺激IUI疗法是否比期待疗法有更好的结局。】We have reported a three-fold improvement in livebirths. This improvement suggests a need to reconsider the NICE recommendation that clinics should not offer IUI and instead should consider IVF as first-line treatment for unexplained infertility of more than 2 years duration. 译【据我们报道,活产率提高了三倍。这种改善表明需要重新考虑NICE的建议,即诊所不应提供IUI,而应考虑将IVF作为持续时间超过2年的不明原因不孕症的一线治疗。】This recommendation was based on the findings of two randomised controlled trials that did not report benefit, but had different populations, different interventions, and higher attrition rates than our study. 译【该建议基于两项随机对照试验的发现,这两项试验没有报告受益,但与我们的研究相比,具有不同的人群、不同的干预措施和更高的损耗率。】Few clinics have heeded the NICE guidance and there have been calls for randomised controlled trials of IUI compared with EM. Our study is one such randomised controlled trial. 译【很少有临床注意到NICE指南,并且有人呼吁对IUI进行与EM相比的随机对照试验。我们的研究就是这样一个随机对照试验。】For couples with unexplained infertility and an unfavourable prediction score, IUI with ovarian stimulation could be offered as a safe and cost-effective first-line strategy.译【对于不明原因不孕和预测评分不佳的夫妇,IUI联合卵巢刺激可以作为一种安全且经济的一线策略。】